Idaho’s Expanding Care Deserts
As OB specialists leave, family doctors and midwives are left handling riskier pregnancies without nearby support.
Idaho’s specialist safety net is unraveling. Since Dobbs, 114 OBGYNs have exited obstetric practice, with only 20 arriving. With maternal-fetal medicine or OBGYN consults now hours away, family doctors and certified nurse midwives increasingly manage high-risk pregnancies, coordinate delayed transfers, and deliver in under-resourced settings.
Scope limits, legal exposure, and thin on-call coverage compound burnout and liability. Longstanding ties between rural clinicians and urban specialists have unraveled, shrinking real-time consultation and transfer options. Fewer specialists don’t just mean longer drives; they mean riskier births for everyone—patients, babies, and clinicians alike.
Idaho’s Geography of Risk
Drive times to your OBGYN
-
![]()
<30 Minutes to Care
Often the longest acceptable drive for prenatal care, yet still a barrier. Missed visits mean early complications may go unchecked, from gestational diabetes to preeclampsia. Distance also weakens continuity of care and the trusting provider–patient relationships that support healthy pregnancies.
-
![]()
<60 Minutes to Care
At one hour, families enter a “maternity care desert.” Late arrivals increase emergency births, while under-equipped facilities may handle deliveries. Many patients cut prenatal visits, especially low-income earners, compounding risks. Stress, isolation, and anxiety during pregnancy grow heavier at this distance.
-
![]()
<90 Minutes to Care
At 90 minutes, maternal morbidity and mortality rise. Unattended roadside births, hemorrhage, preterm labor, and untreated eclampsia become more likely. Families often relocate temporarily for birth, while emergency services strain. Inequities widen, disproportionately affecting rural, low-income, and racially marginalized communities.
-
![]()
<120 Minutes to Care
Two-hour drives create catastrophic risks: roadside deliveries, delayed treatment for emergencies, and inaccessibility of specialists. Families frequently relocate before delivery, incurring steep financial and emotional costs. Local providers face impossible situations, compounding stress and burnout.
-
![]()
150+ Minutes to Care
All the risks of a two-hour drive to maternity care also apply at 150 minutes. In Idaho, this is not just theoretical; some rural residents live this reality. While these areas are sparsely populated, their isolation underscores how profoundly cut off families can be from essential, life-saving care.
Miles Matter
For many Idahoans, access to maternity care depends on weather, road conditions, and the availability of services in nearby towns—sometimes only on select days. Those living farthest out face added barriers: the ability to take time off work, the reliability of their vehicle, or the cost of frequent trips.
While not every challenge is immediately life-threatening, some are, and together they create serious risks and heavy burdens for pregnant patients.
Bonners Ferry
In Idaho’s most overburdened critical-access hospital community, residents drive upwards of three hours roundtrip to Coeur d’Alene, where they have access to 11 OBGYNs who are responsible for over 100,000 other adult women. Wait times for routine gynecologic care now run 5–6 months, with problem visits scheduling out 2–3 months. Initial prenatal visits are 1–2 months out, meaning many pregnancy conditions are going undiagnosed and untreated for far too long. Closer care options are available in Montana, but Medicaid coverage does not extend out of state.

Orofino
Orofino’s FMOBs serve the Clearwater, Lochsa and Selway River valleys—nearly 8000 sq. miles. First prenatal visits are conveniently scheduled within 1-2 weeks; however, with no maternal-fetal medicine specialists, high-risk pregnancies are referred to Spokane or Coeur d’Alene. Not all patients can afford these recurring trips, so Orofino clinicians must take on riskier deliveries. Medicaid patients predominate here, and with already thin margins, funding cuts are likely to be devastating to pregnant patients' healthcare access.

Challis
The drive to Salmon for obstetrical care is over an hour in good travel conditions, but the mountainous terrain in winter can prove dangerous and impassable. It’s also remote, meaning a lack of passers by—or cell service—for help in case of emergency. Challis lacks a comprehensive Emergency Department, meaning that even the safety net for miscarriage treatment or birth complications is 50 miles distant. There are two family physicians providing obstetrical care, with only one trained in cesarean deliveries in Salmon, meaning care availability is stretched thin.

Boise
The Treasure Valley offers the best care access—including the most OBGYNs, the state’s only full-time care for high-risk pregnancies, the shortest drives, and safest road conditions—yet, even there, it takes up to nine months for a gynecological appointment and 6-8 weeks for an initial prenatal screening, with demand for care outpacing supply. The Medicaid coverage rate here runs between 17 and 25 percent, and with recent Medicaid cuts, more providers are refusing such coverage, leaving care out of reach for many.

Rural Idahoans Face Longer Drives, Longer Waits, and Fewer Options
Between 2022 and 2024, Idaho lost 114 OB-GYNs, with only 20 arriving to replace them. This exodus—which directly coincides with the implementation of Idaho’s abortion bans—disproportionately impacts rural Idahoans in myriad ways.
Urban concentration: 85% of OBGYNs now work in seven counties
Rural deserts: Just 23 OBGYNs remain to serve 569,000 rural residents across 37 counties
Longer drives: Many rural Idahoans now travel 60–120 minutes for prenatal and delivery care, compounding risk if complications arise
Lost Options: Three labor and delivery departments have closed since 2023, with more on the brink
Longer waits: Routine gynecologic appointments increasingly take 3–12 months statewide
2025
Jama Network OpenChange in Number of OB/GYN Physicians Practicing Obstetrics After the Dobbs Decision
Idaho’s OBGYN Crisis: A System in Collapse
A 2025 study reveals a sharp decline in Idaho’s OBGYN workforce—driven largely by restrictive abortion laws. In the period from 2022 to 2024:
43% of OBGYNs stopped practicing obstetrics in Idaho
114 providers left; only 20 new ones arrived, meaning a net loss of 35%
OBGYN availability fell from 2.2 to 1.4 per 10,000 Idaho women
None of the departing physicians relocated to states with similarly severe abortion restrictions
Recruitment has slowed; OB positions that once attracted dozens of applicants now see few or none
Idaho is now among the lowest-ranked states for OB-GYN access
A Snapshot of the OBGYN Exodus
From 2011–2022, Southwest Idaho saw modest, roughly balanced OBGYN arrivals and departures. In 2023—with the onset of abortion bans—the trend snapped. Departures surged to nearly 30 while new hires collapsed to zero. For physicians who stay in Idaho, this means unsafe call schedules, shuttered services, and escalating burnout. For patients, it means months-long waits, fewer prenatal appointments, long drives for delivery, and diminished emergency coverage—especially in rural counties. The Southwest region is emblematic of the rest of the state, shifting from shortage to crisis.
What is an MFM?
Maternal–fetal medicine doctors (MFMs) manage high-risk pregnancies. They treat complex maternal conditions like high blood pressure, diabetes, heart or kidney disease, autoimmune illness, or substance use. They also manage fetal or placental issues like poor growth, birth defects, multiples, or a low-lying placenta. MFMs handle problems such as prior preterm birth or loss, a weak cervix, or early labor. They address infectious exposures, do advanced testing (like detailed ultrasound or amniocentesis), and coordinate deliveries. When care is only available across state lines, insurance and Medicaid often require prior authorization and network-gap exceptions—creating delays.
What is an FMOB?
FMOBs—family physicians with obstetrics training—care for patients before, during, and after pregnancy. They provide prenatal visits, deliver babies, manage low- to moderate-risk pregnancies, treat common complications, and continue postpartum and newborn care. Across rural Idaho, they’re often the only clinicians delivering, stabilizing emergencies, and arranging transfers when risk escalates. As OBGYN and MFM specialists leave Idaho and labor units close, FMOBs keep care local, offer continuity for families, and serve as the bridge to distant hospitals. FMOBs are the only obstetrical care in Orofino, Grangeville, McCall, Mountain Home, and Salmon.
Miles to an MFM
Distance shapes pregnancy in Idaho. Only the small green pockets can reach a maternal fetal medicine specialist within 30 minutes; most towns are hours away from such care. Idaho’s MFM coverage has thinned to the Boise area, with only limited availability in Coeur d’Alene. For patients statewide, that means hours of travel for scans, delayed referrals, fewer consults, and fragmented care. Telehealth helps, but can’t replace hands-on exams and procedures—raising risks for mothers and babies when complications evolve quickly.
Data: JAMA Network Open. 2025;8(7):e2524893. Doi:10.1001/jamanetworkopen.2025.24893
Cartography by Jon Waldrup. digitalforestry@gmail.com
Sources: ESRI, USGS, Idaho State Tax Commission, US Census Bureau, Idaho Transportation Department
These maps of Idaho represent lands stewarded since time immemorial by many Indigenous nations, including the Coeur d’Alene, Nez Perce, Shoshone-Bannock, Shoshone-Paiute, Kootenai, Kalispel, Cayuse, Umatilla, and Walla Walla peoples, among others. These communities have cared for the mountains, rivers, and plains of what is now called Idaho for countless generations, and they continue to live, create, and lead here today. We honor their sovereignty, resilience, and ongoing relationship with these lands and waters.
-
![]()
Your Body Is a Battleground
Legal barriers to reproductive healthcare over time.
-
![]()
Women Weaving Community
Historical contributions of women to our community.
-
![]()
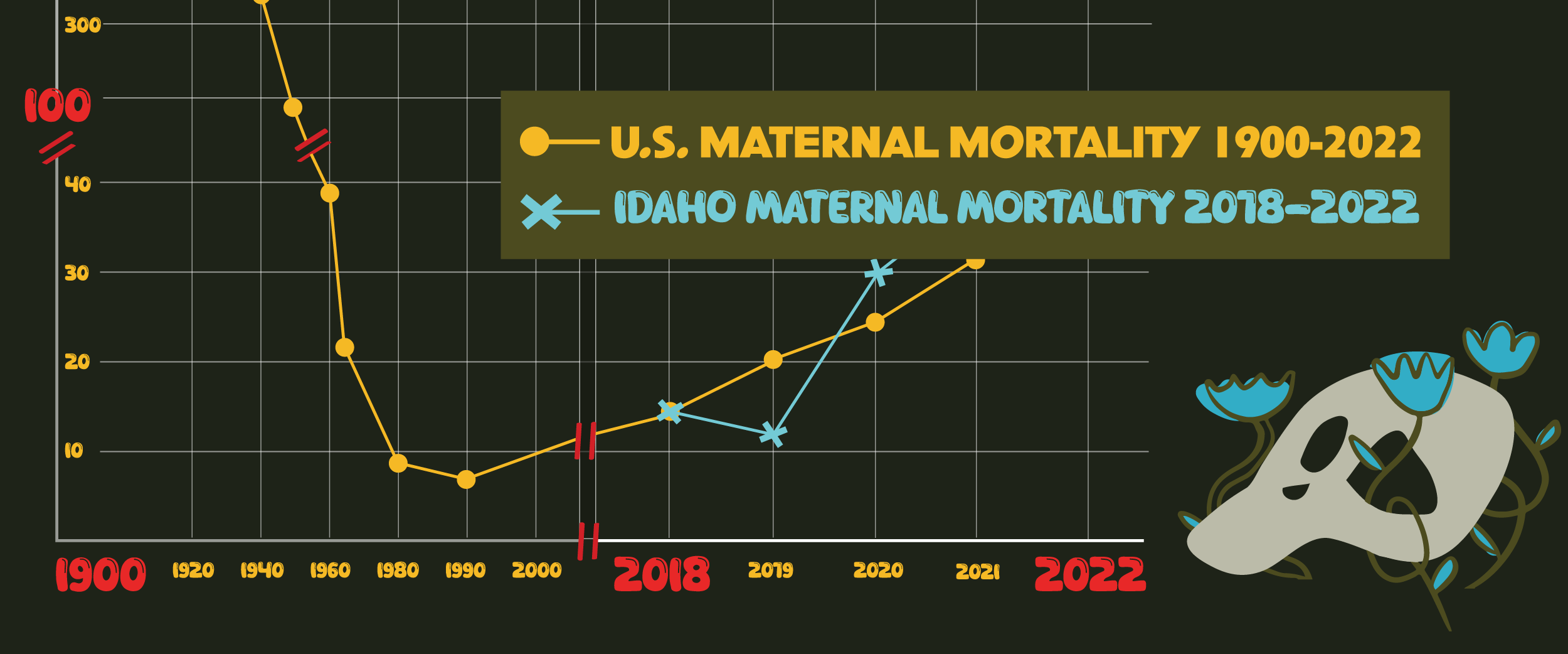
Maternal Mortality in the US
A look at maternal mortality rates and contributing factors.
-
![]()
Shame, Stigma, Silence
The moral and social dimensions of gynecology.
-
![]()
Undervalued, Under-treated, Under-Studied
How we systemically undervalue women's healthcare.
-
![]()
(CO)Operation
How different care options play out in one's life.
-
![]()
Map of Gynecologia
The previously uncharted wilderness of Women’s healthcare.
-
![]()
The Future
What do you want to see for the future in the state of Idaho?
-
![]()
BGH Birth Stories
Personal accounts and birth stories at Bonner General Hospital.
-
![]()
Idaho's Expanding Care Deserts
As OB specialists leave, family doctors and midwives are left handling riskier pregnancies without nearby support